
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
eBook (68 pages):
– Adhesions; Capsular snapping;
– Fibular head and lateral meniscus subluxations / biomechanics, pathophysiology, clinical diagnosis, imaging, manual treatment, Self-Adhesiolysis by patient, rehabilitation… = for understanding.
Movie (47 min):
– The Diagnosis (clinical, visual, palpatory… without imaging): adhesions – capsular trappings – meniscus subluxations – fibular head subluxations (essential and original);
– The Manual Treatment by Dynamic Adhesiolysis® and capsular release;
– The self-manipulations needed for the patient, etc. = for an immediate application.
Both non-surgical and post-surgical forms of knee pain are common complaints, and can be particularly debilitating for manual laborers or those who play sport regularly. Medical treatments for the condition are relatively ineffective, as are the numerous manual therapies that have so far been put forward.
This booklet is based on an open, 26-month study published in 2008. Included in the study were 81 military personnel, all of whom played sport regularly, and who had been suffering from anterolateral knee pain for approximately 13 months. Within this group, we identified a proximal tibiofibular (PTF) origin in 73% of cases, which was subsequently confirmed by a radiological analysis. After manipulation of the subluxation of the head of the fibula (guided by x-ray analysis and not by classical osteopathic examination, which too often gives divergent results), 85% of patients were able to return to sport, of whom 30% within 48 hours wearing a support stocking. We deduced from this that the head of the fibula acts as the knee’s safety valve, and that for its manipulation to be effective, one should absolutely not follow the diagnosis classically proposed in osteopathy teaching.
In 2010 we successfully treated 5 failed cases from the aforementioned group using Dynamic Manual Adhesiolysis®, having discovered, via dynamic ultrasound, adhesions between the Vastus lateralis, Rectus femoris and Vastus intermedius muscles of the Quadriceps. Following manual restoration of the movement of these fasciae during the ultrasound test, clinical improvement was immediate. We have since discovered these adhesions in every case we have examined, and treat them prior to each reduction of the fibula. When the failure of the treatment persists (in around 20% of cases), the dynamic ultrasound often reveals subluxation of the lateral meniscus (manipulated according to classical teaching), or a pathological plica or femoropatellar capsular snapping during bending of the knee; these lesions are often associated. These forms of impingement can be accessed via manipulations which we refer to as “capsular liberation”.
If this is ineffective, we generally subsequently discover a surgical lesion which had not initially been identified. Dynamic ultrasound examination (which is easy to learn for any osteopath who knows what he or she is looking for) has led us to select the manipulations which we currently employ, and we are counting on the osteopath community to improve these further.
We are proposing a visual and palpatory osteopathic diagnosis of 4 types of lesion approachable to our manipulations, because not all the practitioners have access to X-rays and ultrasound. Those who will get into the dynamic ultrasound will progress faster, and finally do more easily without or discover new applications (spine, pelvis). We wish that our name is no longer associated to new signs and techniques, because the ego is a hurdle in the evolution of our wonderful discipline. I hope that our successors will remember it.
 We believe that adhesions of the musculotendinous fascia of the anterolateral aspect of the thigh which are frequently caused by a malposition of the fibular head, often associated with lateral subluxation of the meniscus, and the patello-femoral synovial adhesions are at the origin of most of the non-surgical mechanical knee pain. If untreated, these results in uneven weight distribution of the knee, damage the menisci, and predispose to serious knee sprain. With time, the fragile state of the knee would have repercussions on the ankle, and affect walking, and also give rise to pelvis and spine dysfunction.
We believe that adhesions of the musculotendinous fascia of the anterolateral aspect of the thigh which are frequently caused by a malposition of the fibular head, often associated with lateral subluxation of the meniscus, and the patello-femoral synovial adhesions are at the origin of most of the non-surgical mechanical knee pain. If untreated, these results in uneven weight distribution of the knee, damage the menisci, and predispose to serious knee sprain. With time, the fragile state of the knee would have repercussions on the ankle, and affect walking, and also give rise to pelvis and spine dysfunction.
Plain radiography allows us to classify 4 major types of subluxation of the fibular head: antero-superior (50%), postero-superior (33%), and antero-inferior, and postero-inferior.
The dynamic sonography shows us the real-time dysfunction of the musculotendinous fascia, the pathologic plicae or subpatellar snapping, and the lateral subluxation of the meniscus.
Our study made us revise the clinical and osteopathic examination for a more reliable clinical diagnosis, and to provide an effective manual therapeutic method: Dynamic Manual Adhesiolysis®.
By following our algorithm, the novice practitioner should achieve quick results. The more experienced practitioner will certainly improve on our current method. We hope that health care practitioners will have the opportunity to validate our observations.
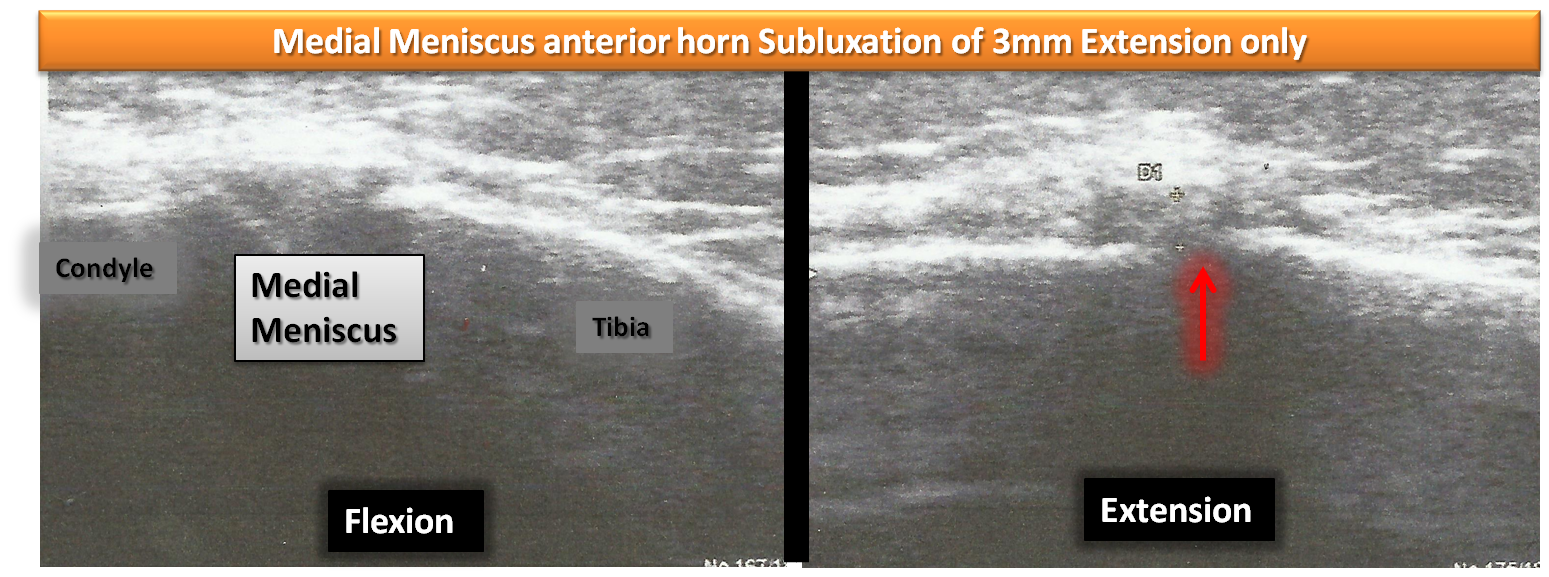
Subluxations of the medial meniscus occur mainly during forced knee flexion. If the meniscus is not surgical, its normalization (then self-manipulation) is facilitated by “unsticking” the Semi-tendinous / Gracilis / Sartoriustendons from hypoderm and Medial Collateral Ligament. The reasons, manipulations and thigh temporary supportive contention will be explained later.
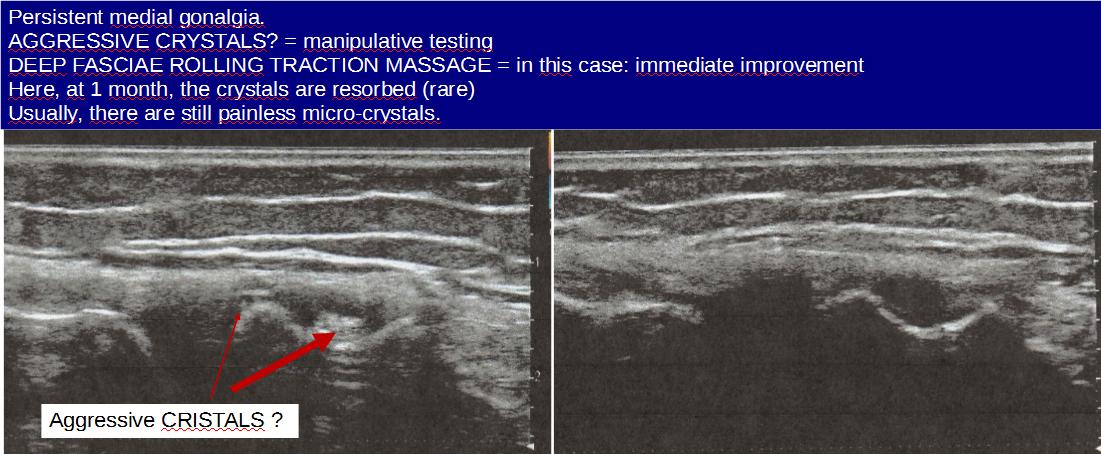
Recent discovery responsible for persistent gonalgia : aggressive micro crystals
Free excerpts of the movie:
Former videos (naive quality) in French